67 Hyperkalemia
# Hyperkalemia
- Check BS (hyperglycemia/DKA/HHS), CK, LDH
- increased AST may be a clue towards cell lysis as cause
- Re-check K, CBC (thrombocytosis, hemolysis, WBC > 50k)
- EKG
- PVR
- Medication review: ACEi/ARB, NSAIDs, -azole, heparin/LMWH, TMP/SMX, tacrolimus, spiro
- Consider telemetry
- Consider other causes:
- Increased production: TLS (KcUP), rhabdo, high K diet
- Decreased excretion: AKI/CKD, hypOaldosteronism, volume depletion, type 4 RTA
- Cellular shift: insulin def, beta-blockers, cell death, acidemia
- Treatment:
- r/o urinary obstruction and hyperglycemia
- 1L NS, followed by IV Lasix (Topf's dose: Cr x 20)
- Regular insulin 10U IV + D50 (25g glucose) if BS < 250
- Patiromer
- Calcium gluconate - 3g IV over 10 mins (lasts 30-60 mins)
- Calcium chloride has faster onset, but can cause tissue necrosis (should be infused via central access)
- LR preferable if no metabolic acidosis
- Low K diet (exclude from fluids, TPN, etc.)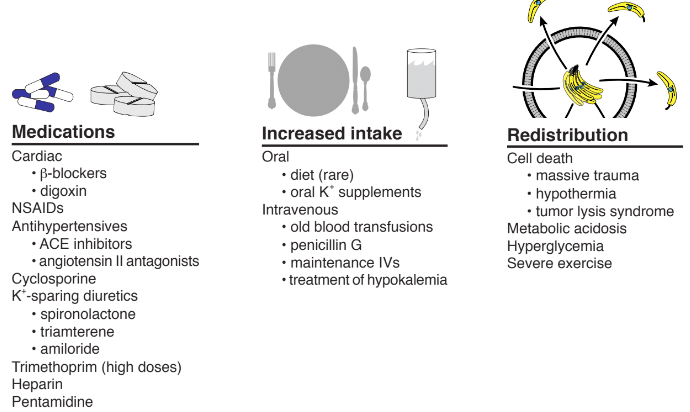
67.1 EKG Changes

Peaked T-waves
Flattening/loss of P wave (loss of atrial contraction)
Increased PR interval and widening of QRS complex
If severe, 'sine wave' pattern
Severe hyperkalemia (e.g. K > 7) can occur without obvious EKG changes Source